"Pan inhibitors permanently and irreversibly stop certain functioning of EGFR. Initial cell studies have indicated these stronger inhibitors can work against the resistant cells with the mutation. To determine whether the T790M mutation leads to resistance to EGFR inhibitors that have different molecular structures and mechanisms, we screened four commercially available EGFR inhibitors (AG1478, cetuximab, erlotinib, and CL-387,785) using cells that were transiently transfected with the delL747–S752 construct and the delL747–S752+ T790M construct. We consistently found that CL-387,785, a specific and irreversible anilinoquinazoline EGFR inhibitor, strongly inhibited EGF-induced phosphorylation While this may not be a valid alternative for many patients, it may make sense for patients whose cancers have been shown to be associated with EGFR."
: E: I. l$ J- E4 Z/ C2 H* c" a! F$ j0 K2 O2 L, ]
"Some recurrent tumors have a common secondary mutation in the EGFR kinase domain, T790M, conferring drug resistance, but in other cases the mechanism underlying acquired resistance is unknown. In studying multiple sites of recurrent NSCLCs, we detected T790M in only a small percentage of tumor cells.... Although gefitinib-resistant clones are cross-resistant to related anilinoquinazolines, they demonstrate sensitivity to a class of irreversible inhibitors of EGFR. These inhibitors also show effective inhibition of signaling by T790M-mutant EGFR and killing of NSCLC cells with the T790M mutation." Kubayashi+ Y4 h. s1 \, O2 {$ _' ^
, ?1 m4 P& g7 h6 KIts success in human studies has been debatable. There have been several trials but none sufficient impressive to move towards FDA approval. Many of these studies did not deal solely with T790M but a variety of patients. Part of the problem may be the company's desire to secure aa drug that is effective overall, and reports testing for the T790M mutation and detailing the drug's impact are strangely difficult to find.
6 V; j6 H, `( _$ N
* L1 K( o/ i8 p8 z' A; k8 l* L/ h
B. HKI 272& D$ N F4 G5 S& n: g; i5 L1 O) S
: s2 S! s, [% j& t& G# D0 K
0 G" k3 {" ~' H3 W/ [One cell study found pan-inhibitor HKI 272 effective with tumor cells in a laboratory setting. "HKI 272 is effective in inhibiting various lung cancer mutations- "HKI-272 is effective in growth inhibition of Ba/F3 cells transformed with EGFRvIII, EGFR-L858R, and EGFR-L858R-T790M." Ji (1)- u# }# n: h% d- D l2 F
- A+ s4 \# m/ W+ n! U1 `( ^% J9 c/ C$ h( E E G9 _$ a
C. Lapanatib
5 {- }9 D7 q* e9 N# i. L
9 m3 p: z3 _. O+ Y: ], T. SA recent study showed promise for a combination of Cetuximab (Erbitux) and Lapatanib (Tykerp),
: |& y% w) B" r- Z1 H. h W T4 g4 }* x/ m5 n0 v
$ T- m) [& w- w2 @# E- ?3 {$ h
9 d- A, E$ z# R% E2 ?, y2 ]: o$ C"In this study, we show that a combination of lapatinib and cetuximab overcomes gefitinib resistance in NSCLC with the T790M mutation. We observed that T790M lung cancer cells were resistant to gefitinib, and Stat3 was persistently activated in the resistant cells. A reversible EGFR and HER2 TKI, lapatinib, decreased Stat3 activation by blocking heterodimerization of EGFR and HER2, which led to a modest increase in the inhibitory effect on gefitinib-resistant T790M cells. In addition to lapatinib, the anti-EGFR antibody, cetuximab, induced down-regulation of EGFR and apoptotic cell death in T790M cells. Finally, combined lapatinib and cetuximab treatment resulted in significantly enhanced cytotoxicity against gefitinib-resistant T790M cells in vitro and in vivo. Taken together, these data suggest that treatment with a combination of lapatinib and cetuximab, which induces dimeric dissociation and EGFR down-regulation, appears to be an effective strategy for treatment of patients with EGFR TKI-resistant NSCLC.") H7 t [/ ]$ w5 ^" l) ]9 j6 P
$ e T/ S z D* H, d
8 v5 ?5 f+ E% v' WBoth Erbitux and Lapatanib are FDA approved drugs, though not specifically approved for this purpose. They can be prescribed off label if a physician chooses.+ h s u; g: K
9 {6 S- k: m$ a3 |7 C
D. Zactima (ZD-6474)
) x* ?9 E) z" }! V: Q8 p& ?$ i$ h; h1 [9 d3 p) K' U
% t7 h: t2 P" J1 A& P+ {
E. BMS 690514
9 v T$ p) X$ D0 r9 z |* b5 ^ t
Only cell studies are available. "BMS-690514, a novel panHER/vascular endothelial growth factor receptor (VEGFR) inhibitor described here, exerted antiproliferative and proapoptotic effects on NSCLC cell lines, with prominent efficacy on H1975 cells expressing the T790M mutation."
" _* c; n" H1 P* V3 A! w* `& v; F: s5 S7 E( F" d% q
|
 老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
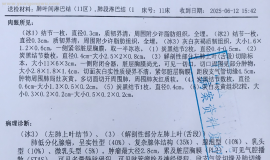
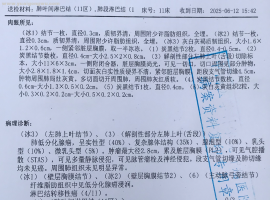
 父亲肺鳞癌,cT3N0M1a,ⅣA,脑转移
父亲2025年6月中旬因为头痛,一侧肢体不灵活入院,做了增强核磁,发现右侧额叶占位(3
父亲肺鳞癌,cT3N0M1a,ⅣA,脑转移
父亲2025年6月中旬因为头痛,一侧肢体不灵活入院,做了增强核磁,发现右侧额叶占位(3
 SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
 希望给没有阅读过的人一些体会
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么
希望给没有阅读过的人一些体会
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么
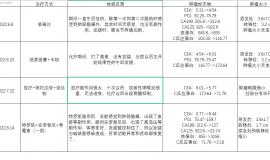
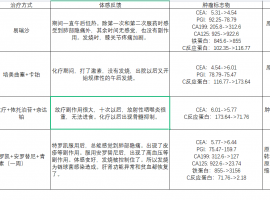
 L858R+S768I+TP53阿法替尼用药半年希
2023.11.23我父亲(63岁)因胸腔积液,呼吸困难,后背疼,声音沙哑入院。此前一个多月
L858R+S768I+TP53阿法替尼用药半年希
2023.11.23我父亲(63岁)因胸腔积液,呼吸困难,后背疼,声音沙哑入院。此前一个多月






 显身卡
显身卡

 高高兴兴是一天,愁眉苦脸还是一天,就看如何选择。生命会随着时间的流失而慢慢远去的,珍惜现在的每一天,过好每一天是最重要的,别给自己吃后悔药。
高高兴兴是一天,愁眉苦脸还是一天,就看如何选择。生命会随着时间的流失而慢慢远去的,珍惜现在的每一天,过好每一天是最重要的,别给自己吃后悔药。